

#169: 🩸 How I Fixed My Dad’s Diabetes Crashes in 4 Weeks
How I used by pharmacology degree, a CGM, diet changes, and one banana to stabilize my dad's blood sugar

Hey Friends,
I just got back from a month in Australia with my dad and I have a story I need to share with you.
It’s personal. It was stressful. And it completely changed how my 78-year-old dad manages his type 1 diabetes.
As a pharmacologist, I’ve spent my career understanding how drugs work in the body. But this was the first time I applied that knowledge to someone I love, in real time, on the road, with no safety net.
The results blew us both away.
💬 In this note:
🩸 How I Fixed My Dad’s Diabetes Crashes in 4 Weeks
📚 Men Explain Things To Me
⚡️ Year of the Rabbit, or Cat?
#169: 🩸 How I Fixed My Dad’s Diabetes Crashes in 4 Weeks

My dad is 78 years old and has type 1 diabetes.
He started as a type 2 diabetic, which eventually developed into insulin dependence.
He does multiple insulin injections a day and wears a continuous glucose monitor (CGM).
I got him on a CGM about a year and a half ago, and that alone was hugely transformative.
Before that, he was doing finger pricks, giving himself way too much insulin, and going into diabetic comas, episodes where his blood sugar would drop so low that his brain essentially stopped functioning.
This. was. terrifying.
He wouldn’t fall asleep exactly.
He’d be in this zombie-like state, kind of there, processing information, but nothing really working.
It’s similar to watching someone who’s had way too much alcohol.
We’ve had to call the paramedics multiple times. They give him a glucose injection and he snaps back. Then he’s on a sugar high because he was just given a ton of glucose. And the roller coaster starts again.

Getting him on the Abbott Libre 3 continuous glucose monitor (CGM) relieved a lot of stress for my mom, for him, and for me.
It sends his blood sugar reading to his phone, my phone, and my mom’s phone in real time.
I absolutely love this device. It is brilliant, easy to use app.
(@Abbot if you want to sponsor my newsletter, please reach out! 🤩)
But it was only step one.
The Deal
Before we left for Australia, I set a rule:
“We’re not going unless you haven’t had a diabetic coma in the last six months. It’s too high risk, something could happen on the plane.”
He was managed that. No crises in a year and a half.
So we went.
And on the flight from Las Vegas to LA before our long-haul to Brisbane, I sat my dad down and said:
“Will you do an experiment with me? Everything we try on this trip, we can change. We can go back to how you were doing things before. But will you be on board and try some of the things I suggest so we can better manage your blood sugar?”
He said yes.
The Roller Coaster Problem
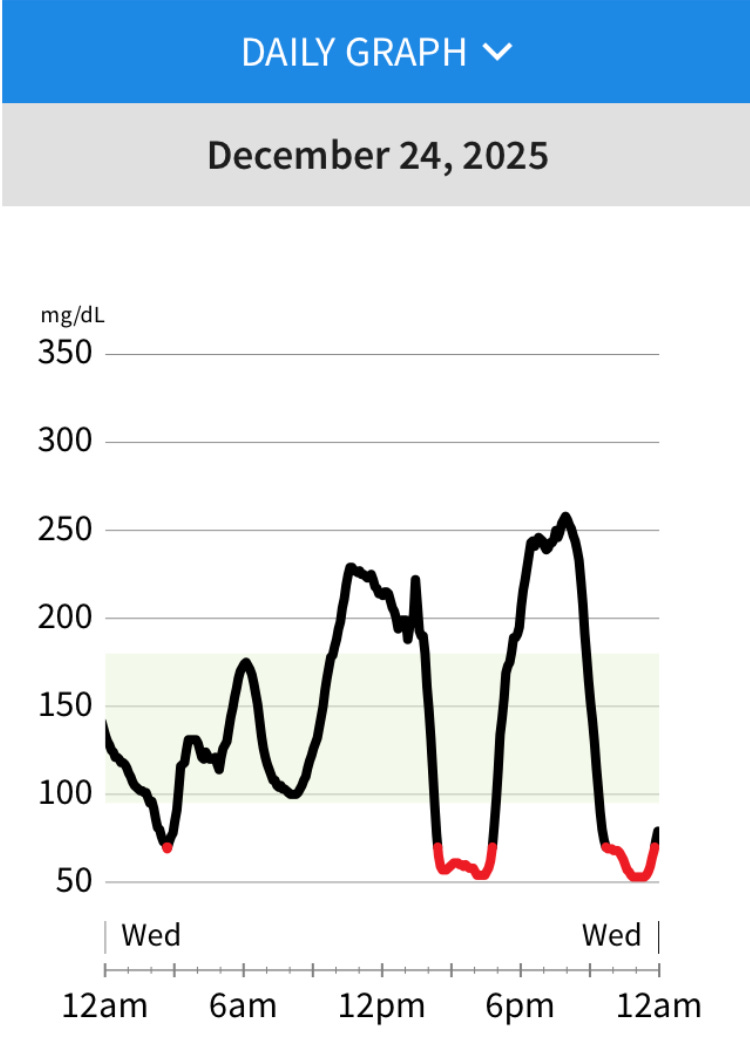
Before our experiment, my dad’s daily blood sugar reading looked like a stock market crash, spike to 300, crash to 60, back to 300, down to 60. A violent roller coaster.
I imagine the feeling was horrible.
What I wanted to see instead was slow, rolling hills as his readings from the CGM.
A flat line would be nearly impossible, but something stable, that was the goal.
His doctor had prescribed 14 units of slow insulin in the morning, 14 at night, and 3 units of fast insulin with every meal.
Based on what I had seen, the crashes, the paramedic calls, the collapses on his walking trail and as a pharmacologist who understands pharmacokinetics, I knew he was taking too much insulin.
⚠️ Disclaimer: I am a pharmacologist, not a medical doctor. This is not medical advice. This was an experiment with an N of 1, my dad, and the results we saw. If you’re going to change medications, you absolutely need to talk to your doctor. I told my dad the same thing: when we get home, we talk to the endocrinologist about every change we made.
The First Test: A 13-Hour Flight
We sat down for a bowl of ramen before the flight. I watched his blood sugar start to skyrocket. We did some fast insulin and brought it down.
Then I said: no more insulin for the rest of the flight. And we’re not eating anything on the plane.
My dad, who has been doing this routine for decades, pushed back.
“I need to do my slow insulin.”
I said, “
Why don’t we just wait and see?”
What happened over those 13 hours was beautiful.
We saw a slow, steady curve decreasing from about 200 down to 100. The fast insulin caught up with the food. The slow insulin from the morning was still working.
No crash.
No panic.
No emergency.
I had proved my first point: the slow insulin lasted longer than he thought.
What 9 Things I Changed (And Why It Worked)
1. Eliminating the Nighttime Insulin Dose
Here’s what I discovered: my dad’s 14 units of slow insulin taken in the morning lasted a full 24 hours.
When he was doing that second dose of 14 units at night, he was stacking insulin
…and crashing in the middle of the night.
He’d wake up stressed, sweaty, disoriented, fumbling around for a soda to bring his blood sugar back up.
That meant terrible sleep, which affected his stress levels, which affected his blood sugar the next day. A vicious cycle.
I said, let’s try just the 14 units in the morning and see what happens.
We did it for the entire month. According to the CGM, how he felt, and how he was sleeping, it was perfect. No more middle-of-the-night crashes.
2. Reducing the Fast Insulin Dose
His doctor recommended 3 units of fast insulin per meal.
I said, let’s be cautious, let’s try 2 units and see what the CGM tells us.
Two units worked for most of the meals we were eating. We avoided those terrifying straight-down arrows on the CGM that signal a rapid blood sugar drop.
3. The Golden Rule: Never Take Insulin Without Eating
This was a non-negotiable.
Before the experiment, my dad would sometimes skip breakfast, take his fast insulin, and go for a three-mile walk carrying weights.
He believed exercise was bringing his blood sugar down. But it was actually the fast insulin on an empty stomach.
This is why he had collapsed on his walking trail, more than once. People found him and had to contact us to get him to the hospital.
New rule: insulin always, always, always goes with food.
Food with slow insulin and fast insulin. No exceptions.
Want to read the rest of this story?
Upgrade to a paid subscription to get the full breakdown of the 9 specific interventions with the science behind them, the insulin adjustments, the diet overhaul, the “emergency bedside banana,” and the dramatic results (reducing 85 blood sugar alerts to only 6 alerts, 15 lbs lost) after 4 weeks and the actionable takeaway summary.
Keep reading with a 7-day free trial
Subscribe to Nina’s Notes to keep reading this post and get 7 days of free access to the full post archives.